Cesarean Section procedure and complications
What is Cesarean Section procedure
Cesarean Section - Surgical CHILDBIRTH. In cesarean (spelled caesarean in countries other than the United States) section, the obstetrician makes an incision through the abdominal wall and the wall of the UTERUS to extract the FETUS. Doctors in the United States perform cesarean section, also called c-section, to deliver 90 percent of breech presentations (fetus is bottom down rather than head down in the uterus) and about 25 percent of pregnancies overall. Most cesarean sections are unplanned though nonemergency, performed because of the mother’s health status, the size of the baby, or the failure of labor to progress. Emergency cesarean section may be necessary when the fetus is in distress.
Though some women feel disappointed or even dismayed to need cesarean delivery, the outcome of healthy baby and healthy mother is the overarching objective. A woman who feels rushed into surgical delivery should discuss alternatives with her obstetrician. Ideally the woman and the obstetrician have had discussions during the course of PRENATAL CARE about the circumstances under which the obstetrician may recommend cesarean section and are in agreement about them.
| COMMON REASONS FOR CESAREAN SECTION | |
|---|---|
| cephalopelvic disproportion | ECLAMPSIA |
| erratic fetal heartbeat | GENITAL HERPES outbreak |
| higher order multiples (triplets or more) | known serious BIRTH DEFECTS |
| known SPINA BIFIDA | macrosomia (very large baby) |
| maternal CARDIOVASCULAR DISEASE (CVD) | maternal HIV/AIDS |
| maternal DIABETES | nonprogressive labor |
| PLACENTA abruptio | placenta previa |
| PREECLAMPSIA | previous CESAREAN SECTION |
| previous uterine surgery | prolapsed UMBILICAL CORD |
Most hospitals allow the woman’s partner to be present in the operating room during nonemergency cesarean delivery. The partner must change into sterile clothing (scrubs) and remain outside the sterile field, usually seated beside the woman’s head; the delivery team will provide clear and specific instruction for the partner. A draped sheet provides a screen to block the woman’s view of the OPERATION as it is taking place. Except in emergency situations when time is crucial, ANESTHESIA is nearly always epidural (injection of the anesthetic DRUG into the space around the SPINAL CORD) or spinal. These forms of anesthesia provide complete PAIN relief for the mother but do not affect the infant. General anesthesia, because the drugs enter the mother’s BLOOD circulation, affects the infant and may suppress BREATHING and HEART RATE.
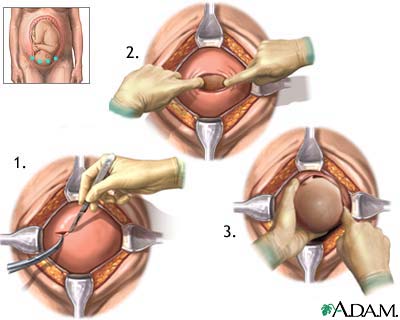
Cesarean Section - Surgical Procedure
After the anesthesia takes effect, the obstetrician makes an incision through the SKIN and abdominal muscles to expose the uterus, then makes an incision through the wall of the uterus to deliver the baby. The most common incision is the low transverse (also called the bikini cut), running horizontally across the lower abdomen just above the pubic BONE about at the pubic hair line. An alternative incision for rapid delivery is the vertical incision, which extends from the umbilicus (belly button) to just above the pubic bone.
The obstetrician first delivers the baby’s head and thoroughly suctions the secretions from theNOSE, MOUTH, and upper THROAT. The pressures and forces of a vaginal delivery would squeeze these secretions from the infant as it passed through the birth canal. Removing the secretions is essential to prepare the airways for breathing. The obstetrician then delivers the rest of the baby and clamps the umbilical cord. The pediatrician examines the baby to assess its breathing and overall health. Often the obstetrician allows the woman’s partner to cut the cord and show the baby to the mother. To this point, the cesarean section takes about 10 minutes.
The rest of the cesarean section takes about 40 minutes and consists of delivering the placenta, repairing the incision into the uterus, and repairing the incision through the abdominal muscles and the skin. The anesthesiologist may administer a sedative to help the mother relax and sleep during this part, after which she goes to the recovery unit until the epidural anesthesia wears off and sensation returns.
Cesarean Section Risks and Complications
The risk for serious complications is very low with cesarean section. Among them are unusual bleeding, blood clots, and INFECTION in the immediate postoperative period, injury to the BLADDER or ureters, and URINARY TRACT INFECTION (UTI). There is also risk, comparable to that of vaginal birth, of injury to the infant.
The path of recovery is substantially longer for cesarean section than for vaginal birth. Most women spend three to five days in the hospital for initial recovery. The doctor will prescribe ANALGESIC MEDICATIONS to relieve pain that are safe for the woman to take while she is BREASTFEEDING. During the first two weeks at home the woman needs to take care of her incision as the doctor instructs. Full recuperation takes six to eight weeks, during which the woman needs help lifting and caring for the baby. However, walking and other physical activities are necessary and important for HEALING as well as to keep the LUNGS clear and to help prevent blood clots.
Long-term complications are rare and are most likely to occur when the cesarean section was an emergency and the obstetrician made a vertical incision. This incision creates weakness in the abdominal wall, the muscles of which have already stretched as a consequence of the pregnancy. Proper care is essential for optimal healing. The risk of incisional HERNIA is higher with the vertical incision than the transverse incision.
Cesarean Section Outlook and Lifestyle Modifications
While the incision is healing the woman needs substantial help carrying and lifting the infant as well as with daily activities. After healing is complete the woman may and should return to full activities, including SEXUAL INTERCOURSE as she desires. Cesarean section does not affect the ability to breastfeed for as long as the woman desires or the potential for becoming pregnant again. Vaginal delivery with subsequent pregnancies (VBAC, or vaginal birth after cesarean) is possible for about two thirds of women who had transverse incisions on the uterus. Most obstetricians consider a vertical incision on the uterus too risky for VBAC because the stress of labor may cause the incisional SCAR on the uterus to rupture.
For further discussion of cesarean section, please see the overview section “The Reproductive System.”
See also APGAR SCORE; POSTOPERATIVE PROCEDURES; PREOPERATIVE PROCEDURES; SURGERY BENEFIT AND RISK ASSESSMENT.