Ovarian Cancer - symptoms, signs, stages, diagnosis and treatment
What is Ovarian Cancer
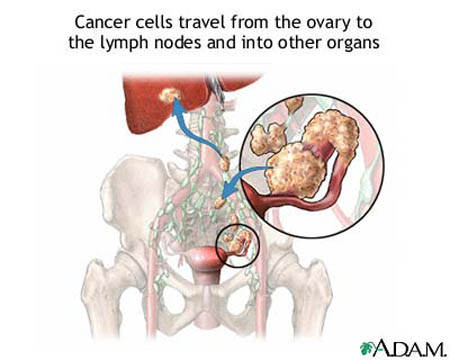
Ovarian Cancer is a malignant (cancerous) tumor that develops in the tissues of the ovary. Ovarian cancer may arise from any of the ovary’s three types of cells-germ, stromal, and epithelial-though about 90 percent of ovarian cancers arise from the ovarian epithelium (the membranous covering of the ovary). Ovarian epithelial cancer occurs most commonly in women over age 60 (after MENOPAUSE). Though tumors are typically noncancerous or cancerous, ovarian epithelial tumors may straddle the border. Doctors classify such tumors as low malignant potential (LMP); though cancerous these tumors grow slowly, have little propensity to metastasize (spread) and usually respond very well to treatment. Ovarian epithelial cancer that develops in women under age 60 is often LMP. Ovarian germ cell cancer and ovarian stromal cell cancer are rare; they are more likely to occur in women under age 50 (before menopause).
Doctors in the United States diagnose ovarian cancer in about 22,000 women each year. Because ovarian cancer typically causes few symptoms until it has metastasized (spread), the prognosis (outlook) for ovarian cancer overall is rather bleak. However, early diagnosis allows successful treatment and a promising outlook. Any woman who has her OVARIES is vulnerable to ovarian cancer, even if she has had a HYSTERECTOMY (OPERATION to remove the UTERUS). Bilateral OOPHORECTOMY (operation to remove both ovaries) ends the risk for ovarian cancer, though it remains possible for epithelial cancer very much like ovarian cancer to develop in the peritoneum, the membranous lining of the abdominal cavity.
Symptoms of Ovarian Cancer and Diagnostic Path
Early symptoms of ovarian cancer are often generalized and vague. Both the woman and her doctor commonly mistake them for symptoms of gastrointestinal disorders. These early symptoms may include
- sensation of abdominal bloating
- abdominal swelling
- unexplained weight gain
- changes in bowel habits (CONSTIPATION or DIARRHEA)
- urinary urgency
As ovarian cancer progresses, symptoms become more specific and include
- pelvic, abdominal, or low BACK PAIN
- unexplained weight loss
- unusual vaginal bleeding
- fatigue and general sense of not feeling well (malaise)
- persistent gastrointestinal symptoms (NAUSEA, VOMITING, diarrhea, or constipation) that do not vary with eating patterns
The diagnostic path includes comprehensive medical examination including PELVIC EXAMINATION, BLOOD tests (cell count and differentiation as well as CA-125), abdominal ULTRASOUND or COMPUTED TOMOGRAPHY (CT) SCAN, and often COLONOSCOPY.
Blood levels of the protein CA-125 are often elevated in moderate to advanced ovarian cancer though not in early ovarian cancer. As well, numerous noncancerous conditions can elevate CA-125 blood levels. Though the doctor may consider the CA-125 level among the diagnostic indicators, it does not alone confirm or rule out diagnosis of ovarian cancer. Other tumor markers include ALPHA-FETOPROTEIN (AFP), HUMAN CHORIONIC GONADOTROPIN (hCG), and CARCINOEMBRYONIC ANTIGEN (CEA).
Because benign tumors and cysts of the ovaries are common, noninvasive diagnostic procedures often cannot determine whether an ovarian growth is cancerous or noncancerous. The only certain diagnostic procedure is laparoscopy or laparotomy, both of which are surgical operations to enter the abdominal cavity, to view the ovary and remove samples of tissue (biopsy). Laparoscopy is a MINIMALLY INVASIVE SURGERY in which the surgeon uses several small incisions through which he or she inserts an endoscope (flexible, lighted viewing instrument) and specialized instruments to visualize the ovary via display on a monitor. Laparotomy is an OPEN SURGERY in which the surgeon makes a substantial incision through the SKIN in the abdomen and examines the ovary directly.
The pathologist who examines the tissue samples determines the type of cancer cells that are present and assesses the extent to which they are likely to have spread to locations outside the ovary. The results of this assessment, called STAGING AND GRADING OF CANCER, help guide treatment decisions. The pathologist also may revise the stage or grade may change after surgery to remove the cancer, depending on the surgeon’s findings and the character of the cancer cells within the tumor.
Ovarian Cancer Stages
| BASIC STAGING OF OVARIAN CANCER | ||
|---|---|---|
| Stage | Meaning | Treatment Options |
| low malignant potential (LMP) | tumor is borderline cancerous and slow growing | surgery to remove the involved ovary (unilateral OOPHORECTOMY) |
| stage 1 | cancer remains confined to a local tumor in one ovary | surgery (bilateral salpingo-oophorectomy, total HYSTERECTOMY, omentectomy, and lymphadenectomy) intraperitoneal CHEMOTHERAPY, RADIATION THERAPY with follow-up single DRUG chemotherapy, or combination (multiple drug) chemotherapy |
| stage 2 | cancer involves both OVARIES or has spread to the FALLOPIAN TUBES, UTERUS, or tissue within the pelvis | surgery (bilateral salpingo-oophorectomy, total hysterectomy, omentectomy, and LYMPH NODE dissection) combination chemotherapy, four to six cycles |
| stage 3 | cancer has spread to other organs in the abdomen, the peritoneum, and abdominal LYMPH nodes | surgery (bilateral salpingo-oophorectomy, total hysterectomy, omentectomy, and lymph node dissection) and debulking surgery combination chemotherapy, four to six cycles |
| stage 4 | cancer has spread to distant organs | debulking surgery combination chemotherapy, multiple cycles “second look” surgery to remove remaining cancerous tissue |
| stage 4/recurrent | cancer has returned after treatment | combination chemotherapy IMMUNOTHERAPY clinical trial of appropriate investigational new treatments high-DOSE chemotherapy with autologous bone marrow therapy (STEM CELL support) palliative surgery for symptom relief |
Ovarian Cancer Treatment Options and Outlook
The treatment of first choice for nearly all ovarian cancers is surgery to remove the ovary that contains the tumor. In all ovarian cancers except LMP, surgery also includes removal of the rest of the pelvic reproductive organs—both ovaries, both FALLOPIAN TUBES, uterus, and CERVIX—as well as the omentum (a layer of fatty tissue that covers the interior of the peritoneum) and nearby LYMPH nodes (lymphadenectomy). Because ovarian cancer tends to spread in layers of cells that cover the pelvic or abdominal structures, the surgeon removes as much of it as possible through a procedure called debulking. Debulking may also involve removing segments of the SMALL INTESTINE.
Most women also receive adjuvant therapy (follow-up treatment) with CHEMOTHERAPY, RADIATION THERAPY, or both. Treatment with a single chemotherapy agent is often sufficient to treat early stage 1 ovarian cancer, though many oncologists prefer combination chemotherapy or radiation therapy with single-agent chemotherapy after. Multiple cycles of combination chemotherapy are the current standard of treatment for stage 2 through stage 4/recurrent ovarian cancer. Some chemotherapy agents are available in oral forms (pills), which a woman can take at home, and others are available only in intravenous injectable forms, which require administration at a chemotherapy center.
| CHEMOTHERAPY AGENTS TO TREAT OVARIAN CANCER | |
|---|---|
| cisplatin | doxorubicin |
| etoposide | ifosfamide |
| melphalan | paclitaxel |
| topotecan | |
High-dose chemotherapy with autologous BONE MARROW therapy, also called STEM CELL support, is often effective in providing short-term REMISSION in stage 4 ovarian cancer. However, many cancer experts question whether the high risk and cost of this treatment ultimately improves a woman’s QUALITY OF LIFE and LIFE EXPECTANCY. For many women, investigational treatments provide equal or better results with significantly less severe side effects and complications.
Because the spread of ovarian cancer within the abdominal cavity is so diffuse, early detection and treatment are particularly essential. Surgery is most effective when the tumor remains confined to the ovary; treatment is most effective when the surgeon is able to remove all of the cancer. The outlook for remission with early treatment is very good. Later stage ovarian cancer is difficult to control because the surgeon cannot remove all of the cancer. Chemotherapy provides highly effective treatment though side effects can be significant. Later stage ovarian cancer has a tendency to recur after remission, though each period of remission may last three to five years.
Risk Factors and Preventive Measures
The primary risk factors for ovarian cancer are age greater than 60 years and family history of ovarian cancer, especially among first-degree relatives (mother, daughter, sister). Women who carry the BRCA-1/BRCA-2 GENE mutations have especially high risk, though not the certainty, to develop ovarian cancer. Some women who have such high risk choose prophylactic oophorectomy (surgery to remove the ovaries) when they reach the end of their childbearing years or menopause as a means for reducing their risk.
The causes of ovarian cancer are unclear, though there appear to be hormonal correlations. Women who carry at least one pregnancy to delivery, breastfeed, or take oral contraceptives (birth control pills) for longer than three years, or have a TUBAL LIGATION or a total hysterectomy (surgery to remove the uterus and cervix) for reasons other than cancer appear significantly less likely to develop ovarian cancer. Lifestyle factors such as the fat content of the diet and the frequency of physical exercise also correlate to the risk for ovarian cancer, with the risk much lower in women who eat a low-fat diet and get daily physical exercise (minimum 30 to 60 minutes). Cigarette smoking raises the risk for ovarian cancer, as it does for many cancers.
Though many ovarian tumors are difficult to palpate (feel), health experts recommend routine pelvic examination as a means of possible early detection of ovarian cancer. However, the PAP TEST that often accompanies a pelvic examination, while very effective for detecting early CERVICAL CANCER, does not detect ovarian cancer. The schedule of examination varies with age and health status, though women at high risk for ovarian cancer should have annual pelvic examinations.
See also BREAST CANCER; CANCER TREATMENT OPTIONS AND DECISIONS; COLORECTAL CANCER; ENDOMETRIAL CANCER; ENDOSCOPY; SURGERY BENEFIT AND RISK ASSESSMENT.