Lymphoma - symptoms and treatment
What is Lymphoma
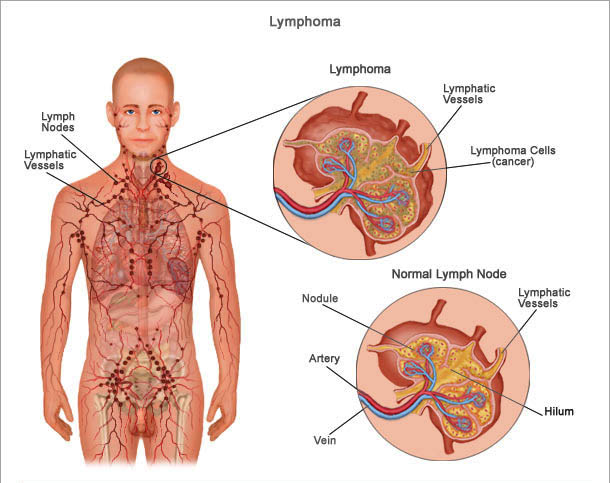
Lymphoma is a type of CANCER that affects the hematopoietic functions of the LYMPH system that results in the uncontrolled proliferation of lymphocytes, the type of LEUKOCYTE (white BLOOD cell) that the lymph tissues primarily produce. The lymphocytes congregate in the lymph tissues to form tumors.
LYMPHOMA VS. LEUKEMIA
LEUKEMIA and LYMPHOMA are both cancers that can affect the lymphocytes. However, leukemia is a CANCER of the BONE MARROW that alters the development and proliferation of lymphocytes that enter the BLOOD circulation. Lymphoma is a cancer of the lymphatic tissues that produce lymphocytes.
Though there are nearly three dozen identified types of lymphoma doctors assign them to one of two major categories, Hodgkin’s lymphoma and non-Hodgkin’s lymphoma. Doctors diagnose about 60,000 people with lymphoma in the United States each year. Lymphoma is the fifth most common kind of cancer among American adults and the third most common kind of cancer among children.
How Lymphoma Develops
Lymphomas originate in the reticuloendothelial or clone cells in the lymph structures that produce lymphocytes, notably the lymph nodes and the SPLEEN. Most lymphomas affect B-cell lymphocytes (B-cells) though some affect T-cell lymphocytes (T-cells). Hodgkin’s lymphoma involves a specific kind of B-cell called a Reed-Sternberg cell. In all lymphomas, the affected lymphocytes proliferate and migrate to lymph tissues, such as lymph nodes and the spleen. The lymphocytes cluster into tumorous formations that drain the NUTRIENTS and other resources healthy cells require, causing the healthy cells to die and allowing the cancerous lymphocytes to continue proliferating.
A key marker for the extent and severity of lymphoma is whether tumors are present on only one side or on both sides of the DIAPHRAGM. Lymphomas present only on one side of the diaphragm (either above or below) tend to be less aggressive than those that are present in LYMPH NODE regions on both sides of the diaphragm, as well as more responsive to treatment (particularly those above the diaphragm). Cancerous lymphocytes can also metastasize to other kinds of tissues throughout the body, primarily traveling through the lymphatic system. The most common sites for lymphoma METASTASIS outside the lymphatic system are the BRAIN, SKIN, BONE, and BONE MARROW. However, because the lymphatic network extends throughout the interstitial tissues, metastases in advanced disease can appear anywhere.
Hodgkin’s Lymphoma
Hodgkin’s lymphoma, also called Hodgkin’s disease, accounts for about 15 percent of diagnosed lymphomas. It most commonly affects people between ages 16 to 34 and over age 55. The presence of specifically abnormal B-cells, Reed-Sternberg cells, is the hallmark of Hodgkin’s lymphoma. There are five identified subtypes of Hodgkin’s lymphoma:
- lymphocyte-predominant (also called nodular lymphocyte predominance)
- nodular sclerosis
- lymphocyte-rich (also called classical)
- mixed cellularity
- lymphocyte-depleted
Treatment regimens and prognoses differ for each subtype. Nodular sclerosis Hodgkin’s lymphoma is the most common subtype, accounting for about two thirds of diagnoses, and tends to be moderately progressive. Lymphocyte-predominant Hodgkin’s lymphoma tends to progress slowly; lymphocyte-depleted Hodgkin’s lymphoma tends to be quite aggressive with rapid progression and frequent metastasis to organs outside the lymphatic system. In general, the higher the number of Reed-Sternberg cells, the more aggressive the cancer.
Non-Hodgkin’s Lymphoma
The non-Hodgkin’s lymphomas account for about 85 percent of diagnosed lymphoma and most commonly affect people over age 60, though can develop at any age. There are several dozen subtypes of non-Hodgkin’s lymphoma, currently classified according to the type of tumor (also called a neoplasm) and its characteristics. Doctors further classify non-Hodgkin’s lymphomas as to whether they are aggressive (rapidly growing)-high or intermediate grade-or indolent (slow growing)-low grade.
| NON-HODGKIN’S LYMPHOMA SUBTYPES | |
|---|---|
| AIDS-related | anaplastic large cell |
| angioimmunoblastic | blastic natural killer (NK) |
| BONE | Burkitt’s |
| CENTRAL NERVOUS SYSTEM (CNS) | cutaneous T-cell |
| diffuse large cell | diffuse small noncleaved cell |
| eyelid | follicular |
| immunoblastic | lymphoblastic |
| lymphoplasmacytic | mantle cell |
| marginal zone | MUCOSA-ASSOCIATED LYMPHOID TISSUE (MALT) |
| mycosis fungoides | nasal NK/T |
| nodal marginal zone | ocular (EYE) |
| small lymphocytic | splenic marginal zone |
Symptoms of Lymphoma and Diagnostic Path
Many people do not have symptoms of lymphoma at the time of diagnosis. Rather, the doctor detects characteristic abnormalities in diagnostic blood tests conducted for other reasons, often as part of a ROUTINE MEDICAL EXAMINATION. When symptoms are present they can be vague and generalized, typical of common viral infections though they tend to persist or recur rather than resolving. Such symptoms may include
- painless swellings in the lymph nodes, most noticeable in the axillae (underarms), neck, or groin (LYMPHADENOPATHY)
- unexplained, frequent fevers
- unintended or unexplained weight loss
- profuse sweating at night
- tiredness, fatigue, or lethargy
- unexplained, generalized itching (PRURITUS)
The diagnostic path begins with the doctor’s physical examination, which may reveal SPLENOMEGALY (enlarged spleen) or detect enlarged lymph nodes beneath the collarbone or in the abdomen. Diagnostic blood tests and bone marrow biopsy demonstrate the proliferation of lymphocytes. Other diagnostic procedures the oncologist may conduct include tissue biopsy of swellings, COMPUTED TOMOGRAPHY (CT) SCAN or MAGNETIC RESONANCE IMAGING (MRI) to detect the presence of tumors deep within the body, POSITRON EMISSION TOMOGRAPHY (PET) SCAN to examine the lymphatic network, and specialized immunocytology tests to determine the subtype of lymphoma. Based on the diagnostic findings the oncologist assesses the status of the lymphoma, assigning it a stage classification. Oncologists further designate a grade for non-Hodgkin’s lymphoma that characterizes the level of aggressiveness. These assessments determine the appropriate treatment regimens and help valuate the prognosis (likelihood of REMISSION and survival).
Lymphoma Treatment Options and Outlook
Treatment regimens depend on the subtype, stage, and for non-Hodgkin’s lymphomas the grade of the cancer as well as the person’s age and overall health status. The typical treatment approaches, often administered in combinations, include
- RADIATION THERAPY, either above the diaphragm only (mantle field radiation) or from the neck to the pelvis (total nodal irradiation)
- CHEMOTHERAPY
- IMMUNOTHERAPY, also called biological response modifier therapy, including monoclonal antibody (MAb) therapy
- BONE MARROW TRANSPLANTATION and peripheral blood stem cell transplantation (PBSCT)
- watchful waiting for indolent (slow-growing and asymptomatic) lymphomas
| LYMPHOMA STAGING (HODGKIN’S AND NON-HODGKIN’S) | |
|---|---|
| Stage | Characteristics |
| stage 1 | early disease involves only a single LYMPH NODE region |
| stage 2 | locally advanced disease involves two or more lymph node regions on one side of the DIAPHRAGM |
| stage 3 | advanced disease involves two or more lymph node regions on both sides of the diaphragm |
| stage 4 | widely disseminated disease involves multiple lymph node regions and METASTASIS to other organs such as the BONE or BRAIN |
| A | no symptoms at time of diagnosis (asymptomatic) |
| B | symptoms present at time of diagnosis |
| E | lymphoma is present in an organ outside the lymphatic system with no lymph node involvement |
Treatment results in at least one remission for most kinds of lymphoma. Many people experience extended remissions with few recurrences, and some people experience such long-term remissions as to have the oncologist consider the lymphoma cured. Other lymphomas are more resistant to treatment. Some chemotherapy drugs are effective as single agents, though more commonly oncologists prescribe chemotherapy drugs in combinations that target specific types of lymphoma. Many treatment regimens are cycles that repeat over several months to a year. Numerous complications resulting from treatment may occur, and vary with the treatment regimen, type and stage of lymphoma, and person’s age and general health status.
| CHEMOTHERAPY DRUGS USED TO TREAT LYMPHOMA | |
|---|---|
| 5-fluorouracil | bleomycin |
| carmustine | chlorambucil |
| cisplatin | cyclophosphamide |
| cytarabine | dexamethasone |
| doxorubicin | etoposide |
| fludarabine | fluoxymesterone |
| hydroxydaunomycin | ifosfamide |
| melphalan | methotrexate |
| mitoxantrone | pentostatin |
| prednisone | prednisone |
| procarbazine | rituximab |
| tositumomab | vincristine |
Risk Factors and Preventive Measures
Researchers do not know what causes lymphoma, though a number of environmental factors appear to increase the risk for developing these forms of cancer. The most significant risk is for people who receive IMMUNOSUPPRESSIVE THERAPY after ORGAN TRANSPLANTATION, who are 100 times more likely to develop non-Hodgkin’s lymphoma. Other suspected risk factors include
- HIV/AIDS
- INFECTION with human T-lymphocytic virus 1 (HTLV-1), EPSTEIN-BARR VIRUS, or human herpesvirus 8 (HHV-8)
- infection with HELICOBACTER PYLORI, the BACTERIA believed responsible for STOMACH CANCER
- occupational exposure to benzene
- occupational exposure to agricultural pesticides and herbicides, notably organophosphates and chlorophenols
- first-degree relatives (parents, siblings, children) who have lymphoma
- chromosomal TRANSLOCATION and other abnormalities
However, researchers do not know the extent to which these factors influence the development of lymphoma. Many people who develop lymphoma have no history of exposure to these factors, and far more people than not who have exposure do not develop lymphoma. Reducing or eliminating exposure to environmental toxins, treating infections such as H. pylori, and maintaining nutritious EATING HABITS can improve health overall. Otherwise, there are no known measures to prevent lymphoma.
See also AMYLOIDOSIS; B-CELL LYMPHOCYTE; CANCER RISK FACTORS; CANCER TREATMENT OPTIONS AND DECISIONS; ENVIRONMENTAL HAZARD EXPOSURE; ERYTHROPOIETIN (EPO); LEUKEMIA; LIFESTYLE AND HEALTH; MULTIPLE MYELOMA; NATURAL KILLER (NK) CELL; SIGNS AND SYMPTOMS OF CANCER; SMOKING AND HEALTH; STAGING AND GRADING OF CANCER.