Infertility - male and female - what is, causes, symptoms and treatment
What is Infertility and Definition
Infertility - the inability to conceive or maintain a PREGNANCY. Infertility may be transitory (relate to a specific set of circumstances), treatable, or permanent. Infertility affects about 10 percent of Americans who attempt pregnancy.
There are numerous possible causes of infertility that can affect any of the various stages in the process of CONCEPTION. Causes may affect the woman, the man, or the couple in equal distribution. One of the most significant is the woman’s age. An increasing number of women in the United States delay starting their families until completing their education and establishing their careers, the average age of first pregnancy is age 30. Though a woman can remain fertile into her late 40s, the likelihood of conception appreciably diminishes each year after age 35.
Infertility is highly emotional for most people. Infertility often comes as a shock, particularly for younger people who had no reason to suspect they were not fertile. Some people feel guilt or regret about choices made earlier in life in regard to CONTRACEPTION and FAMILY PLANNING. Diagnostic procedures and treatment approaches can be invasive and expensive and are without assurances. Though ASSISTED REPRODUCTIVE TECHNOLOGY (ART) is highly advanced and makes pregnancy possible for thousands of couples every year, it nonetheless is unable to help two thirds of couples who cannot conceive.
Female factor infertility
In female factor infertility the reason for infertility rests with the woman. A third of infertility circumstances arise from female factors. Ovulatory dysfunction is the most common of them and may result from age, genetics, health conditions, or medical treatments. Blocked FALLOPIAN TUBES are also common. Previous ECTOPIC PREGNANCY, abdominal or pelvic surgery, and complications from untreated SEXUALLY TRANSMITTED DISEASES (STDS) may SCAR and otherwise damage the fallopian tubes. Congenital anomalies of the reproductive organs, such as malformations of the UTERUS, may prevent implantation. EATING DISORDERS such as anorexia nervosa and OBESITY influence the body’s endocrine functions and OVULATION. Cigarette smoking, excessive ALCOHOL consumption, and substance abuse also affect FERTILITY.
| FEMALE INFERTILITY FACTORS | |
|---|---|
| age over 35 | excessive ALCOHOL use |
| anorexia nervosa | CHEMOTHERAPY |
| cigarette smoking | CUSHING’S SYNDROME |
| DIABETES | ENDOMETRIOSIS |
| OBESITY | OVARIAN CYST |
| PELVIC INFLAMMATORY DISEASE (PID) | PITUITARY GLAND dysfunction |
| POLYCYSTIC OVARY SYNDROME (PCOS) | PREMATURE OVARIAN FAILURE (POF) |
| previous ECTOPIC PREGNANCY | SICKLE CELL DISEASE |
| RADIATION THERAPY | TURNER’S SYNDROME |
| substance abuse | UTERINE FIBROIDS |
| untreated HYPOTHYROIDISM | uterine malformations |
Male factor infertility
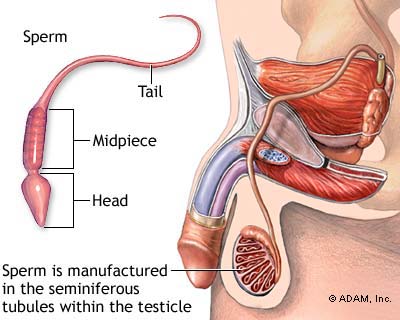
In male factor infertility the reason for infertility rests with the man. A third of infertility circumstances arise from male factors. Male infertility factors may result from problems with spermatogenesis (production of SPERM), SEMEN production, ERECTION and EJACULATION, sperm count, sperm morphology (structure), and sperm motility (movement). Body temperature and scrotal temperature are crucial for spermatogenesis and sperm survival. Circumstances that prevent the SCROTUM from dropping, such as tight clothing, or sustained exposure to heat, such as sauna or hot tub use, may affect sperm viability. Such effects may be temporary or permanent. Viral infections such as the MUMPS and bacterial EPIDIDYMITIS may damage or destroy testicular tissue. CHROMOSOMAL DISORDERS such as KLINEFELTER’S SYNDROME and endocrine disorders may affect TESTOSTERONE production. Congenital absence of the VAS DEFERENS, which often occurs in men who have CYSTIC FIBROSIS, prevents sperm from leaving the TESTICLES.
| MALE INFERTILITY FACTORS | |
|---|---|
| agricultural pesticide exposure | ATHEROSCLEROSIS |
| CHEMOTHERAPY | chronic ORCHITIS |
| chronic PROSTATITIS | chronic URETHRITIS |
| cigarette smoking | CRYPTORCHIDISM |
| CUSHING’S SYNDROME | CYSTIC FIBROSIS |
| DIABETES | DOWN SYNDROME |
| ERECTILE DYSFUNCTION | excessive ALCOHOL consumption |
| HYDROCELE | KLINEFELTER’S SYNDROME |
| HYPOGONADISM | low SPERM count |
| low SEMEN volume | malformed sperm |
| low sperm motility | prolonged elevated body temperature |
| OBESITY | RADIATION THERAPY |
| RETROGRADE EJACULATION | SICKLE CELL DISEASE |
| SPERMATOCELE | substance abuse |
| TESTICULAR CANCER | testicular trauma |
| untreated EPISPADIAS | untreated HYPOSPADIAS |
| VARICOCELE | viral or bacterial EPIDIDYMITIS |
Combined factor infertility
In combined factor infertility the reason for infertility results from the unique combination of factors each partner brings to the couple. A third of infertility circumstances arise from combined factors or remain unknown in their origin. Combined factors may be elements that, on their own, would not be sufficient to prevent conception. In particular combinations, however, these elements result in infertility. The woman’s IMMUNE SYSTEM may generate antibodies that attack the man’s sperm. Combined factor infertility is often the most difficult to sort out and treat.
Symptoms of Infertility and Diagnostic Path
The primary symptom of infertility is the absence of pregnancy after one year of unprotected SEXUAL INTERCOURSE when pregnancy is the desired outcome. The diagnostic path begins with comprehensive medical examination, including PELVIC EXAMINATION for women, and detailed history of attempts to conceive. Further diagnostic procedures depend on the preliminary findings and suspicions, though typically include laboratory tests for STDs, BLOOD tests for antibodies and HORMONE levels for the woman, and semen analysis for the man.
Additional diagnostic procedures for the woman may include
- basal body temperature journaling over several months to assess ovulation
- pelvic or transvaginal ULTRASOUND to examine the OVARIES and reproductive organs
- analysis of vaginal fluids to assess acidity (pH) and mucus
- hysterosalpingogram, a contrast medium X-RAY examination of the uterus and fallopian tubes
- karyotyping to detect chromosomal abnormalities such as TURNER’S SYNDROME
- exploratory laparoscopy to visually examine the internal pelvic structures
Additional diagnostic procedures for the man may include
- blood tests to measure hormone levels
- scrotal ultrasound to detect HYDROCELE, VARICOCELE, or SPERMATOCELE
- karyotyping to detect chromosomal abnormalities such as Klinefelter’s syndrome
Infertility Treatment Options and Outlook
Treatment targets the identified or suspected cause. Basic approaches include frequent sexual intercourse, sexual positions that support conception, and timing sexual intercourse with ovulation. These basic measures result in conception within two years in about a third of couples. Other straightforward solutions may include treatment for infections or endocrine disorders (such as previously undiagnosed HYPOTHYROIDISM or ADRENAL INSUFFICIENCY).
Further treatment is more invasive. In men, such treatment may consist of surgery to repair hydrocele, varicocele, or spermatocele. Testosterone supplementation often improves sperm production and erectile function in men whose blood testosterone levels are low. In women, further treatment may include surgery to correct or repair various situations that contribute to or cause female factor infertility such as abdominal adhesions, ENDOMETRIOSIS, UTERINE FIBROIDS, certain uterine malformations, blocked fallopian tubes, and OVARIAN CYST. Hormone supplementation may regulate the MENSTRUAL CYCLE to encourage or stimulate ovulation (“superovulation”) in women. Some hormones used in this way are off-label (not approved for infertility treatment though approved for other uses) in the United States.
Fertility experts select hormone therapies according to the underlying cause for ovulatory dysfunction, the woman’s age, and any existing health conditions. Hormone treatment for infertility may have serious side effects, risks, and complications, including HOT FLASHES, mood swings, ovarian cyst formation, increased risk for spontaneous ABORTION early in pregnancy (miscarriage), and high risk for pregnancy with multiples (twins or greater). The long-term risks associated with fertility drugs, for the women who take them as well as the children conceived with their assistance, remain uncertain because the drugs have not been in use long enough to allow comprehensive studies.
| MEDICATIONS USED TO STIMULATE OVULATION |
|---|
| bromocriptine |
| cabergoline |
| clomiphene citrate |
| FOLLICLE-STIMULATING HORMONE (FSH) |
| GONADOTROPIN-RELEASING HORMONE (GNRH) analogs |
| human chorionic gonadotropin (hCG) |
| human menopausal gonadotropin (hMG) |
| letrozole |
| metformin |
ART methods to combine sperm and OVA may be appropriate when there are no measures to correct the cause of infertility or attempted treatments have not succeeded.
Risk Factors and Preventive Measures
The primary risk factor for infertility is age. Though the time frame of fertility is clearly defined in women, fertility diminishes to some degree in men as they grow older. Lifestyle risk factors include cigarette smoking, alcohol consumption, environmental hazard exposure (such as pesticides), and obesity. Lifestyle also influences some health risks for infertility such as DIABETES, ATHEROSCLEROSIS, and infection with STDs. Risks for which there are no preventive measures include GENETIC DISORDERS and chromosomal disorders, CONGENITAL ANOMALY of the reproductive organs, POLYCYSTIC OVARY SYNDROME (PCOS), PREMATURE OVARIAN FAILURE (POF), endocrine disorders, and AUTOIMMUNE DISORDERS.
See also ADOPTION; AGING, REPRODUCTIVE AND SEXUAL CHANGES THAT OCCUR WITH; AMENORRHEA; BIRTH DEFECTS; FETAL ALCOHOL SYNDROME; GENITAL TRAUMA; KARYOTYPE; OFF-LABEL USE; PUBERTY; SMOKING AND HEALTH; SMOKING CESSATION; SURGERY BENEFIT AND RISK ASSESSMENT; TUBAL LIGATION; VASECTOMY.