Adhesive Capsulitis shoulder - symptoms, treatment and surgery
What is Adhesive Capsulitis
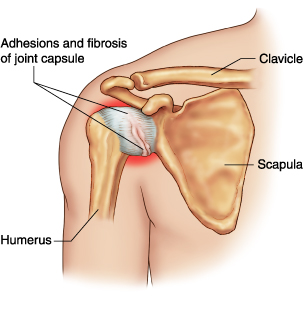
Adhesive Capsulitis shoulder is a condition in which the JOINT capsule of the shoulder joint fuses (adheres) to the head of the humerus (long BONE of the upper arm), causing PAIN and constricting range of motion. Doctors do not know what causes adhesive capsulitis, commonly called frozen shoulder. The condition may be primary, in which there are no contributory conditions, or secondary, in which other conditions exist that may cause changes that allow adhesive capsulitis to develop. Adhesive capsulitis affects women somewhat more frequently than men and typically occurs in people over age 50.
Symptoms of Adhesive Capsulitis and Diagnostic Path
Adhesive capsulitis begins with acute pain in one shoulder that occurs for no obvious cause. Within weeks to months adhesions (scarlike tissue) develop that progressively limit the affected shoulder’s range of motion. Most people first notice restricted movement when trying to reach up and behind, such as combing the HAIR, and when trying to reach back and behind, such as for a wallet in the pocket. The adhesions and range of motion restrictions progress until the person has very limited use of the shoulder. In most people the adhesions gradually lessen and the pain subsides over a period of one to three years. Doctors sometimes refer to the three stages of adhesive capsulitis as freezing, frozen, and thawing.
The pattern of symptoms is generally distinctive enough to allow diagnosis. The doctor may choose to perform diagnostic imaging procedures such as X-RAY or MAGNETIC RESONANCE IMAGING (MRI) to rule out other possible causes of the symptoms.
Adhesive Capsulitis Treatment Options and Outlook
Because adhesive capsulitis is nearly always selflimiting, treatment primarily targets pain relief. Analgesic medications, heat, and PHYSICAL THERAPY in combination may improve range of motion. When symptoms are severe and do not respond to these measures, the doctor may recommend arthroscopic surgery to release the contractures. In most people such surgery relieves the pain and improves range of motion.
The entire course of adhesive capsulitis, treated nonsurgically, typically spans 11⁄2 to 3 years, after which about half of people recover completely with no residual pain or restrictions on range of motion. In some people range of motion improves though remains limited. A few people experience residual pain and contractures that result in longterm disability.
Risk Factors and Preventive Measures
Conditions that appear to increase the risk for adhesive capsulitis include HYPERTHYROIDISM (overactive THYROID GLAND), DIABETES, and HYPERLIPIDEMIA (elevated CHOLESTEROL BLOOD LEVELS and TRIGLYCERIDE BLOOD LEVEL). Adhesive capsulitis is also more common in people who have SPINAL CORD INJURY, PARKINSON’S DISEASE, certain forms of NEUROPATHY, and traumatic injury to the structures of the shoulder. Despite these correlations, doctors do not know what initiates the onset of adhesive capsulitis and therefore do not know what measures may prevent its development.
See also CHRONIC PAIN; COMPLEX REGIONAL PAIN SYNDROME; SURGERY BENEFIT AND RISK ASSESSMENT.